Succinct Version of the Blog Post (TL;DR):
If you have a high deductible plan:
- and haven’t hit your deductible (and are thus price sensitive)
- and have an ailment that can be treated via telemedicine
Then this is a worthwhile tool that helped us out recently: https://www.goodrx.com/treatment. This blog post is also worth reading: https://www.goodrx.com/blog/telemedicine-true-cost-and-telehealth-price-comparison-chart/.
More rambling version of the above:
I recently listened to a podcast in which the podcast interviewee said that the industries most ripe for disruption over the coming decades are 1.) healthcare, 2.) education, and 3.) financial advising.
I’d love to provide the citation, but I frankly don’t remember who said it. I think it may have been the host of the New Retirement Podcast being interviewed on another podcast. If I’m wrong, perhaps someone can correct me.
In any regard, I agree with whoever said that. Those industries are bloated, bureaucratic, and ripe for disruption.
Covid-19 has forced us to re-evaluate many aspects of our lives. Pre-Covid, many of us thought we couldn’t work from home. Post-Covid, I now realize that I can teach reasonably well online using tools like Zoom and Vidgrid (with MS Paint and a simple Wacom tablet). In fact, one student left feedback for me this semester that they preferred the online version of me better than the real version of me because there were fewer Costco tangents in my online lectures. Ouch!!! (I consider myself in good company because Buffett and Munger couldn’t stop raving about them at last year’s Berkshire meeting). I guess my blogging is no different than my teaching; full of superfluous Costco references.
Another thing that Covid has may have taught us is that telemedicine is a viable form of treating some ailments. My primary care physician transitioned to part-time telemedicine during the peak of Covid (though I think he’s since phased it out). Further, a member of the FP clan is seeing a (very expensive) counselor and those sessions transitioned to skype this month.
In May we took a quick trip out of state and a member of the FP clan needed to see a doc for a UTI. Naturally, I checked my insurer’s website to see if there was anyone we could see that was in-network. UMR’s website is miserable, so I called them instead and was told that the answer was “No.” Our out-of-network deductibles/OOP max for my plan are twice the in-network deductibles/OOP max, so that’s a bummer. We were basically on our own; familiar territory for those of us with high deductible plans.
I consulted Google for minute clinics in the area. One was well reviewed so I called them up and asked for pricing information. They quoted me at $85 for the baseline cost of the visit + $30 for an additional test.
I was about to pull the trigger on the local clinic when it occurred to me that my university has been pushing telemedicine on us lately (through brochures and such). The telemedicine company my employer preferred is Teladoc.com, which charges $49 per visit. Not convinced that the visit would appropriately count towards my deductible, I figured I’d Google to see if there were better alternatives. I came across this link: https://www.goodrx.com/treatment from our friends at GoodRx.
Obviously, telemedicine isn’t going to be a solution for all ailments. Just sawed off your leg? A skype call to your doc isn’t going to help you from bleeding to death. Need an appendix removed? Your skype doc isn’t going to be able to help you out there. Too bad because that could have saved us $10k a few years back.
However, there is a reasonably long list of conditions that can be treated via skype. For example, here’s a list of conditions for which GoodRx provides price comparisons (the list is not exhaustive):
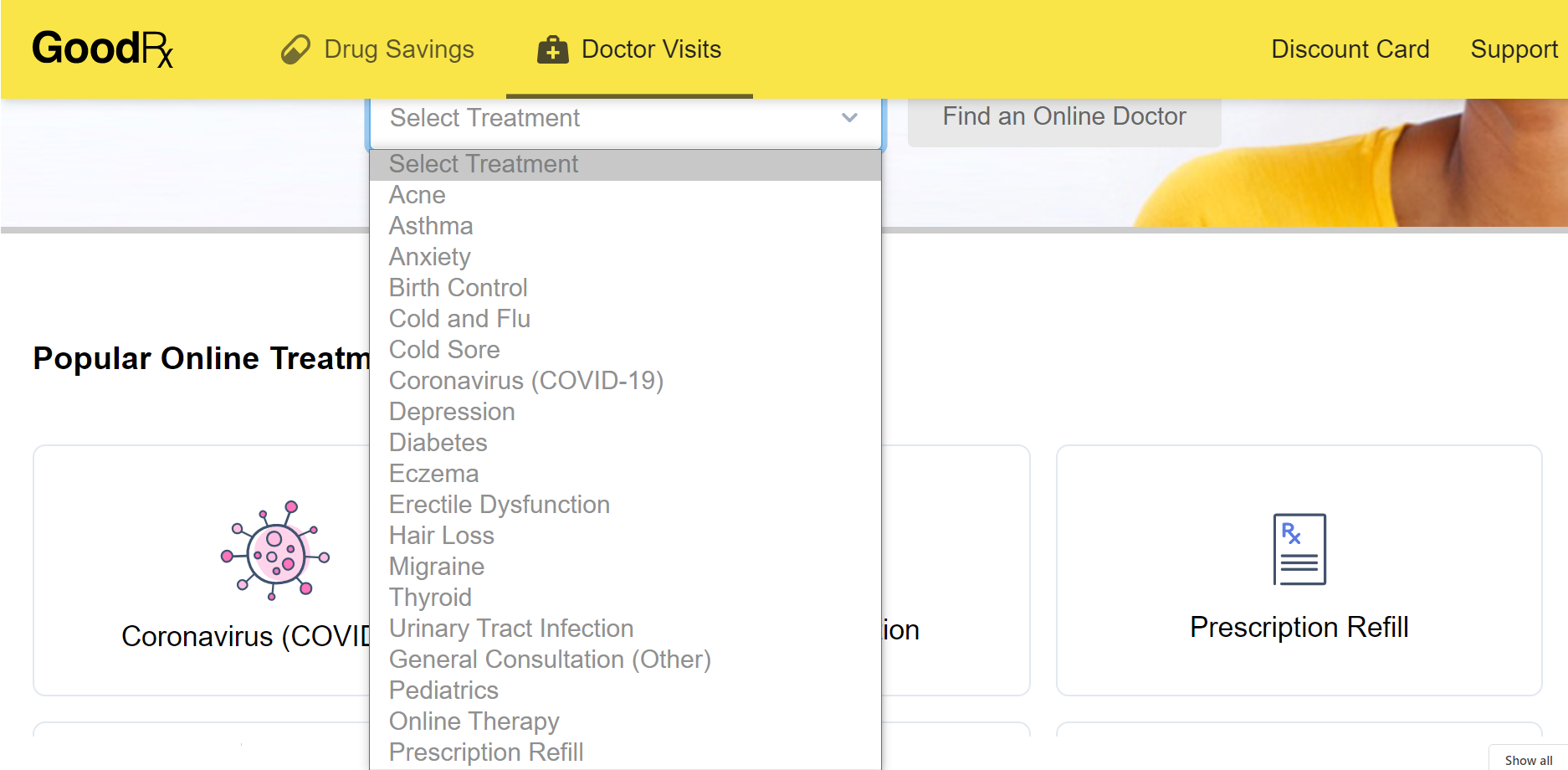 We ended up using this GoodRx comparison tool for the UTI (not #11).
We ended up using this GoodRx comparison tool for the UTI (not #11).
Once you click the relevant ailment, it tells you which provider is cheapest. For the UTI, we got the following result:
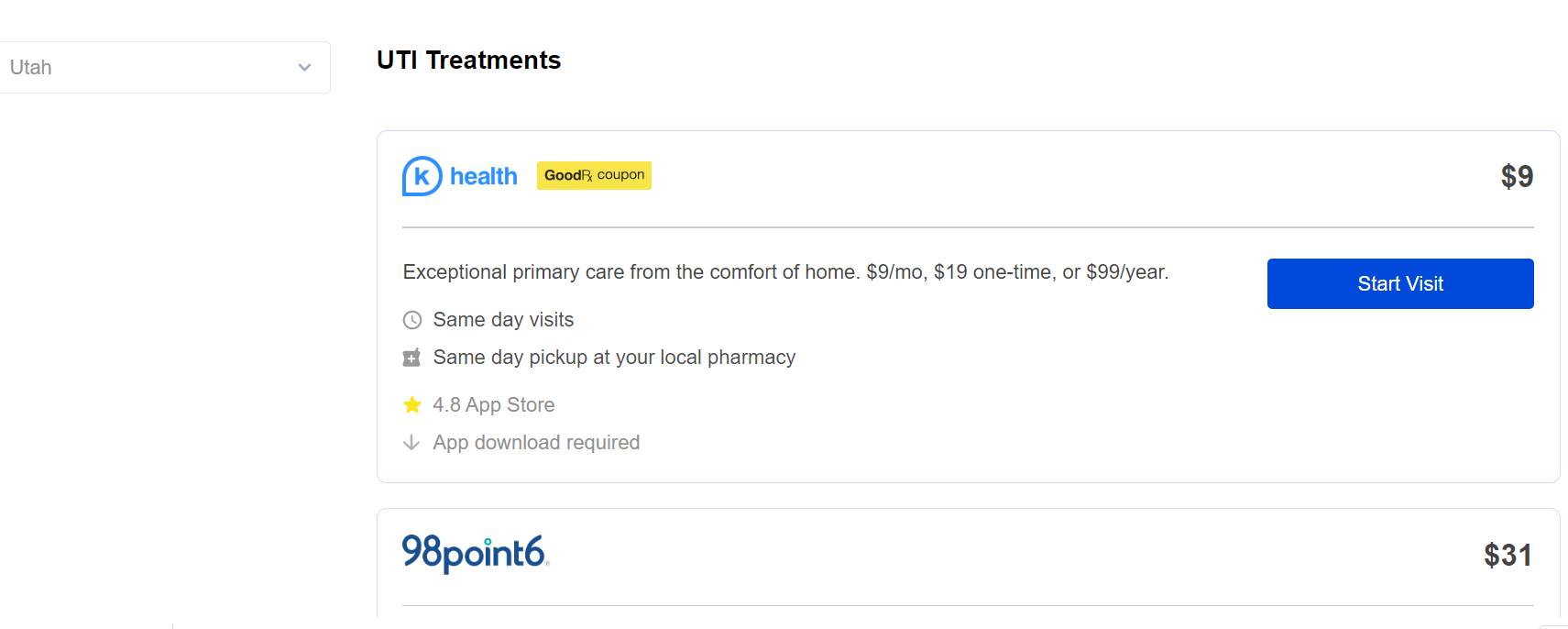
The website/app/company K health, which I’d never heard of before, was the cheapest for us so we went with them. I opted for the $19 one-time charge rather than the $9/month fee because I figured there was some sort of gotcha with the $9/month fee (perhaps I made a mistake).
In any regard, I paid the $19 on their website. They told us to download their app so we did so. We then entered basic info about symptoms via a text-based bot chat. After a 15 minute wait in the queue we proceeded to text chat (no audio/video) with a board certified doc. The doc sent a prescription to the pharmacy down the street which we picked up for $1.36 (less than the price of a Costco hot dog and drink). It was a reasonably slick transaction. I’d definitely do it again.
All in, we’re out $19 + $1.36 = $20.36 to treat a UTI (that’s less than two Costco pizzas after tax!).
Perhaps the doctor readers of the blog will tell chime in that I’ve done something reckless here by not going in to an in-person doc. But the family member has had UTI’s before and says that the symptoms are similar to previous UTI’s.
I can’t imagine how much my parents paid in acne visits for me growing up. If my children have inherited my same misfortune, I will surely try telemedicine for their acne.
Conclusion
Just as Covid has dramatically accelerated our comfort level with Zoom meetings and online learning, it may be the catalyst to accelerate the acceptance of telemedicine. For a select list of ailments, it seems like a no brainer to try since it could potentially save you 80-95% of the cost of a conventional office visit.
This is only our second time using telemedicine; the first was a $10 visit few years back with CHI health. Both times the results were quite favorable.
Audience Poll
Has anyone had any success/horror stories with telemedicine in the past? Please share the company/website/app name if you remember.
I remember being taught in medical school that there’s good evidence that UTIs can be treated via phone calls, but in practice that hasn’t been done because in a traditional setting you can’t get compensated for it. My only hang up with it now is that I usually get a culture- probably more often than I need to, but it’s hard to tell ahead of time if that is going to be necessary.
It will be interesting to see how this sudden change in what is normal will affect the industry. It’s amazing what can happen when they remove one stupid regulation.
Benjamin,
Thanks for the interesting response! What stupid regulation are you referring to?
How much of your job do you think you could viably do over telemedicine as a primary care physician? 10%?
I’d say that 100% of my job could viably be done remotely, but that would compromise the whole fraternity-and-football-stadium undergraduate experience we’ve all come to love. And I’d personally lose my mind being holed up at home.
Unrelated to telemedicine, have you considered practicing concierge medicine? Last time I saw Scott Bean a year or two back he was considering switching to that model for his family practice business. I’d be all-in on an alternative approach to medicine as soon as I don’t have heavily subsidized employer sponsored healthcare.
About a year ago I saw a really interesting video about a family practice doctor in NYC who did cash pay only and had a very well defined price list for ailments. Most ailments were around $40 or so to treat. The doc ran his own practice; no receptionist, no billing department, etc. It seemed like a pretty great way of practicing medicine. I tried to find the link to the video but came up empty.
Probably anywhere from 10 to 30%, perhaps more but again, it changes the “experience”. The regulations that were rolled back were restrictions on telehealth visits as well as some of the regulations surrounding HIPPA. Suddenly, telehealth visits were covered by Medicaid and Medicare, where they weren’t before, as well as by many insurance companies. We also we’re allowed to use things like FaceTime for visits where that would normally not be HIPPA compliant.
There’s an appeal to concierge medicine, but I like my job and my patients too much. I became less satisfied with my employer and didn’t want to live in a small town anymore or do deliveries and inpatient care, I would consider concierge or direct primary care. I don’t love the business side of medicine as much though.
It’s great news that the gov’t and insurance companies have changed the rules with telemedicine. It seems like a win-win proposition for you and your patients.
I’m really glad that you’re liking your job! I can definitely understand the appeal of not having to worry about the business side of things. That would considerably complicate your life.
I’m a neurologist in New York and my clinic switched to 100% telemedicine (in-person visits for emergencies only have to be approved by the department chair), with things re-opening very slowly over the last week. The physical exam is critical in neurology, but I’ve been surprised at how much can be achieved by telemedicine even for complicated neurologic complaints. Maybe not by text message, but certainly by video. That’s not to say that I haven’t been a bit uncomfortable with some of the things I haven’t been able to do on video exam with some patients, but still the percentage of patients for whom it was really completely fine surprised me. And in fact I was able to schedule multiple follow ups in shorter time spans for some patients about whom I was worried and who otherwise wouldn’t have been able to come in to the clinic on, say, a weekly basis. Even for patients who ultimately need to be seen in person, an urgent video visit can still be set up and a preliminary evaluation completed quicker than someone can get into clinic.
Anyway, we went through probably 5 if not 10 years of telemedicine evolution in a few months, and hopefully the good parts are here to stay. I’m sure some of the regulations will be tightened again (ie right now we can do telemedicine across state lines without regard for state of licensing, which I’m sure won’t stick), but I’m hoping the gains in comparable reimbursement aren’t rolled back so it can continue to be a viable option. The ability to use popular non-HIPAA-complaint platforms (like Skype, FaceTime, etc) with patient consent is also a boon to people who are less technologically savvy, and I hope some version of that is retained – lots of my elderly patients have trouble installing and setting up a proprietary telemedicine app, but know how to answer a FaceTime call!
Anyway, thanks for the great posts, Costco cheerleading and all! I’ve definitely “adapted” (stolen) some of your chart styles for my own financial tracking.
Alex,
Thanks for stopping by! I’m impressed that your clinic was able to transition to telemedicine. I never would have guessed that a specialty like neurology would transition reasonably well. Hopefully telemedicine continues to be a viable treatment option going forward. It seems to be a win-win proposition for doctors and patients alike, provided that the regulations & reimbursements can accommodate that reality.
Glad that you’ve found a post or two helpful… I’m happy when others incorporate things I rant about into their lives.
Great idea on comparison shopping tele-medicine. I’ve used Teledoc with great success and currently our insurance pushes us to Amwell. Several of my children have had online sessions with docs during the pandemic, including acne consults. It wouldn’t surprise me if that’s one thing that really keeps up after the pandemic subsides. Blood work still requires going into the lab, though.
Thanks for the feedback! Are all of these Amwell/Teledoc transactions appropriately counting towards your deductible/OOP max? I have little faith that UMR has its act together, but perhaps I’m overly pessimistic…?
Yes, they did, but hey were also the “blessed” tele-medicine options. I’m not sure if they’d be covered the same way if they weren’t. Probably would have been labeled as out-of-network, but I didn’t check.
Good to know; Thanks!